































Tooth autotransplantation is the surgical extraction of a tooth from one location in the alveolus, and implantation at a different position in the ridge. A variation of this is called transalveolar transplantation where a tooth that is severely malpositioned in the correct tooth area is surgically uprighted into a more ideal orientation (see a powerpoint presentation here). Tooth autotransplantation in humans was first reported in the literature by Bjercke and Slagsvold in 1959, and can be used to replace any missing, malpositioned, or damaged tooth. It is a most powerful tool for bone regeneration when immature teeth are transplanted (for example, to replace a tooth and bone in areas of missing teeth and cleft lip), but mature teeth can also be used in certain situations. You can read more about this in our Autotransplantation ProbeTips newsletter.
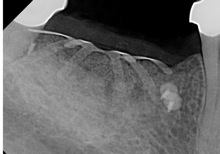
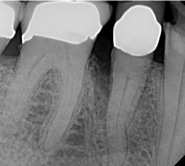
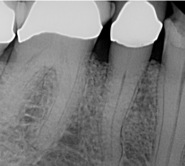
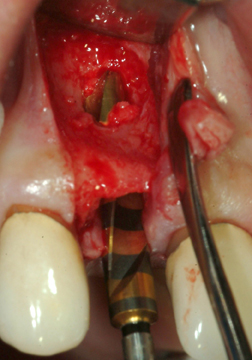
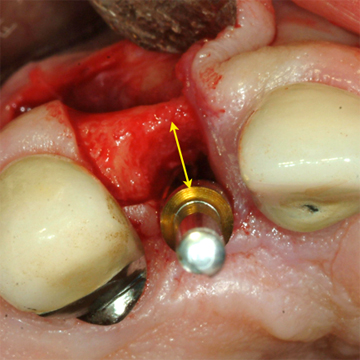
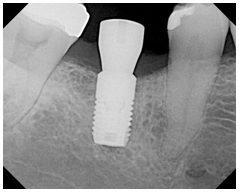
Below is an example of moving a premolar from the lower jaw to a missing front tooth in the upper jaw in a 10 year old boy. This is particularly useful since implants are not available until growth has stopped at age 18 or 20. The transplanted tooth can function for many years, and may even prevent the need for an implant in the front tooth position in the future. The images below are courtesy of Dr. Jim Janakievski and Dr. Gregg Kinzer.